|
In the first of a series of articles about Cane Hill, Simon Cornwell outlines the design and construction of the hospital, explains the unique challenges faced by its architect and how his solution eventually became known as the most complex asylum ever built in the United Kingdom. 
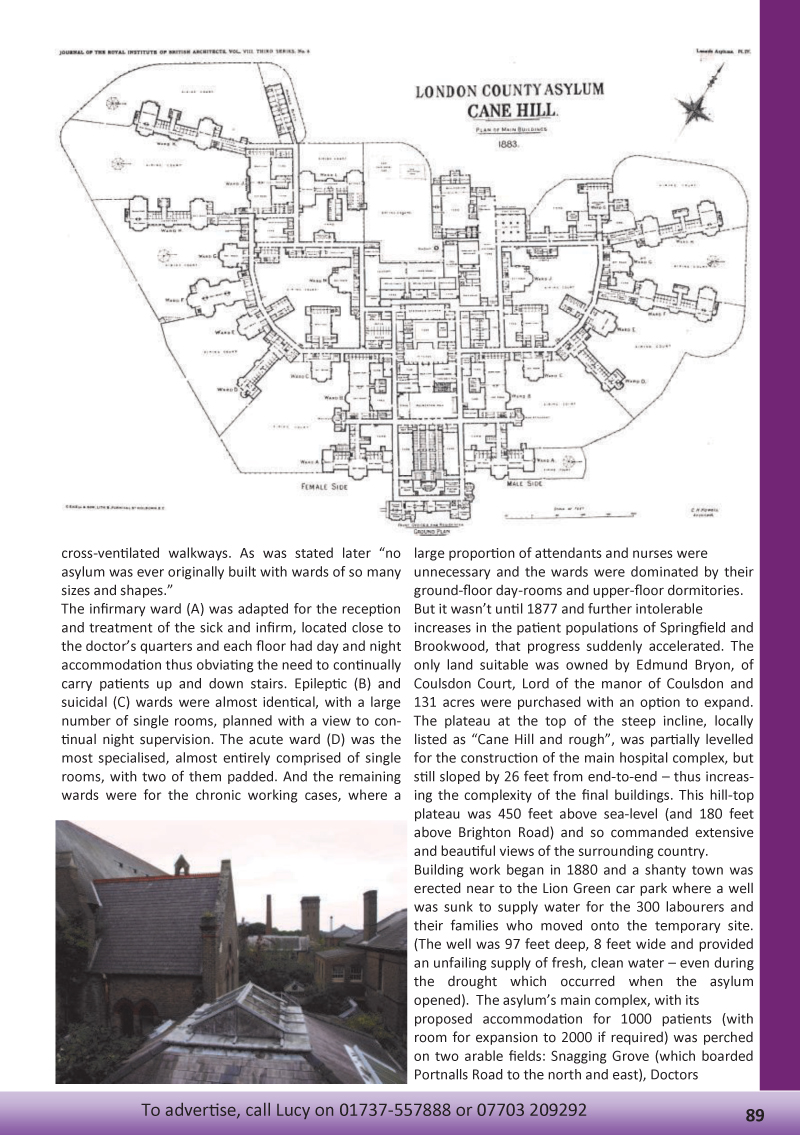
The county architect, Charles Henry Howell FRIBA, gave his honest appraisal of the situation. Talking to the committee of Springfield Hospital in 1875, he’d been asked for his professional opinion: Surrey’s two existing asylums were completely full, despite huge extensions which had doubled their sizes the previous decades and the committee needed further options. His measured conclusion was that Springfield and Brookwood had reached their optimal size. “Such economy would be dearly purchased at the cost of efficiency,” he stated and then proposed the construction of a third county asylum. The committee agreed and implored the county magistrates (the body required by The Lunacy Act of 1845 to provide care and treatment for all pauper lunatics within its jurisdiction) to give permission to build a third asylum. Their long term assessment was damning: without more space "on the grounds of humanity" then the provision of "better care and more frequent cures” would be impossible. Howell’s assessment added considerable weight to the committee’s conclusion. Not only had he designed several asylums in the 1860s and 1870s (including Surrey’s own Brookwood), but he was also the Consulting Architect to the Commissioners in Lunacy. Plus he had other reasons to push for a third institution. His County Surveyor role was part-time, as also (one assumes) was his position on the board of the Commissioners of Lunacy. (There was also still space left in his working week to work as a surveyor for the Norwich Union Insurance Office.) Any new asylum would be a worthy addition to the portfolio of his architectural practice, Howell & Brooks of London, and would provide steady work and income for the next few years. Yet the design of this new institution would not be simple. It would have to economically and humanely house over 1000 patients and no architect had yet created an optimal design. It couldn’t follow the tried-and-tested linear, or ‘corridor’, paradigms which had been the norm in the early decades of the 19th century and had failed so badly when scaled up or expanded. He would’ve also been aware of Florence Nightingale’s "pavilion" system, which had started to influence the design of general hospitals, but had failed when applied to the MAB asylums of Caterham and Leavesden which were greatly criticised. Furthermore Howell would’ve been familiar with the designs of the next wave of proposed asylums and the new ideas emerging from other architects. He was therefore in the ideal position to draw up a bold, new design which would solve the problems inherent in earlier asylums and solidify his name and reputation as an architect. There would’ve been considerable surprise when Howell eventually unveiled his plans revealing an exceptionally bold and adventurous solution. In solving the problem, he returned to the failed, and widely condemned, structure of a semi-circular central corridor with radiating spurs. Yet, on closer inspection, it became clear that he’d solved earlier problems of this pattern (which had found some application in prison design) by enlarging the radius of the central corridor, increasing the spacing between the spurs (now modelled on Nightingale’s pavilion ideas) and placing the hospital’s core within the corridor system. Nothing like it had been seen before. The complexity of the design was daunting. Not only had Howell managed to pack the hospital’s central services within the circumference of the corridor (administration, chapel, Chaplain’s room and library, surgery, recreation hall, sculleries, vegetable-room, officer’s mess room, kitchen, dairy and meat store, steward’s store, bake house, laundry and wash house, engine and boiler house, water tower, coal stores, workshops and mortuary) but he had expanded Nightingale’s pavilion ward ideas into specialised buildings each devoted to a class of mentally ill patient. Radiating from both sides, separated into female and male halves, the wards architecturally represented the needs of the patients treated there: sick and infirm, suicidal, acute, epileptic, chronic etc. No two wards were the same, the buildings met at acute angles, and the two or three storeys blocks intermingled; it was an architectural masterpiece. Howell had already made a name for himself with his epileptic ward design and he now drew up plans for five different ward types, each modelled on the Nightingale pavilion ideal where wards were long and skinny with separate sanitation towers reached by cross-ventilated walkways. As was stated later “no asylum was ever originally built with wards of so many sizes and shapes.” The infirmary ward (A) was adapted for the reception and treatment of the sick and infirm, located close to the doctor’s quarters and each floor had day and night accommodation thus obviating the need to continually carry patients up and down stairs. Epileptic (B) and suicidal (C) wards were almost identical, with a large number of single rooms, planned with a view to continual night supervision. The acute ward (D) was the most specialised, almost entirely comprised of single rooms, with two of them padded. And the remaining wards were for the chronic working cases, where a large proportion of attendants and nurses were unnecessary and the wards were dominated by their ground-floor day-rooms and upper-floor dormitories. But it wasn’t until 1877 and further intolerable increases in the patient populations of Springfield and Brookwood, that progress suddenly accelerated. The only land suitable was owned by Edmund Bryon, of Coulsdon Court, Lord of the manor of Coulsdon and 131 acres were purchased with an option to expand. The plateau at the top of the steep incline, locally listed as “Cane Hill and rough”, was partially levelled for the construction of the main hospital complex, but still sloped by 26 feet from end-to-end – thus increasing the complexity of the final buildings. This hill-top plateau was 450 feet above sea-level (and 180 feet above Brighton Road) and so commanded extensive and beautiful views of the surrounding country. Building work began in 1880 and a shanty town was erected near to the Lion Green car park where a well was sunk to supply water for the 300 labourers and their families who moved onto the temporary site. (The well was 97 feet deep, 8 feet wide and provided an unfailing supply of fresh, clean water – even during the drought which occurred when the asylum opened). The asylum’s main complex, with its proposed accommodation for 1000 patients (with room for expansion to 2000 if required) was perched on two arable fields: Snagging Grove (which boarded Portnalls Road to the north and east), Doctors Common (which ran down to Brighton Road, a convenient east and south-east boundary) and Dunstan’s Wood. Further building saw construction of a small cottage hospital, several gate houses and lodges, a farm and stables. By the end of the construction period in 1882, Howell’s masterpiece stood atop Cane Hill, its non-embellished functional water tower a new local landmark. (The water tower was 107 feet high and the tanks were capable of holding 34,000 gallons of water.) As it was funded by the public purse, all unnecessary elaboration and Victorian embellishment was toned down, but Howell added some novel features. The administration block was completed in a Queen Anne style whilst the Chapel, buried in the heart of the complex, was internally rendered in polychromatic brickwork, designed in Early-English style and could sit 800 patients. The recreation hall was lofty and well proportioned with a gallery (rare for asylums), large stage with Proscenium arch and dressing rooms beneath. By the time of its completion, and after further land purchases, the total hospital estate occupied 151 acres. It was Howell’s crowning achievement. The Third Surrey County Asylum, or Cane Hill as it became known, was opened with considerable acclaim and held up as a possible solution to the many problems of large hospital and asylum design. But Howell, in returning to his role as Consulting Architect, would’ve soon realised that Cane Hill was an over-ambitious solution, as designs by the next generation of asylum architects took up the ‘echelon’ pattern originated by architect George Hine (and used for the later Netherne.) The design of Cane Hill, destined to become the pattern of many future buildings became a unique experiment, an evolutionary dead-end and a footnote in the history of asylum construction and design. Howell never worked on anything as ambitious as Cane Hill again. Yet he would’ve taken some comfort and pride that the doctors and nurses who had just moved into the new hospital, many from other institutions, praised it highly. It had been a slow start: from the grim first meeting at Springfield Hospital in 1875, through to the design and construction of a groundbreaking, bold new institution, but the Third Surrey County Asylum was finally ready to receive it first patients in 1882, when its history as a hospital really begins. Simon Cornwell 


|